Topical corticosteroids Topical corticosteroids are highly effective as treatments for inflammatory skin conditions and a mainstay of treatment for eczema. They inhibit the production and action of inflammatory mediators in the skin. It is important for patients to understand that topical corticosteroids relieve symptoms but do not cure eczema. The appropriate potency for the severity and extent of eczema together with the correct application of topical corticosteroids is essential to reducing the risk of adverse effect. Topical corticosteroids should be used intermittently to control acute eczema exacerbations and reduce inflammation and itching. They are applied in conjunction with emollients but applied at a different time of day to avoid diluting the steroid. The British National Formulary (BNF) (British Medical Association and Royal Pharmaceutical Society of Great Britain, 2009) classifies topical corticosteroids as mild, moderately potent, potent or very potent. Examples of topical corticosteroids available for prescription are listed in Table 9.5; details of constituent elements, such as antimicrobials, are given in the current BNF (British Medical Association and Royal Pharmaceutical Society of Great Britain, 2009).
In general, potent and very potent topical corticosteroids should be reserved for recalcitrant dermatoses and avoided on the face and skin flexures and in children (unless prescribed by a dermatology specialist). The least-potent topical corticosteroid that relieves symptoms should be applied (British Medical Association and Royal Pharmaceutical Society of Great Britain, 2009). Mild and moderately potent topical corticosteroids are associated with few side effects. However, particular care is required in the use of potent and very potent topical corticosteroids. As a guide, clinicians should consider the factors outlined in Table 9.6 when prescribing topical corticosteroids and assessing the risk of side effects.
The current recommendation is to apply topical corticosteroids thinly to the affected area; no more frequently than twice daily and use the least-potent formulation which is fully effective (NICE, 2004a; BNF, 2009). We would advocate the use of the Finger-Tip Unit (FTU) here to enable more precise measurement of the topical steroid being used. Further deatils are given later. Systemic side effects are not common and occur through skin absorption and can rarely cause adrenal suppression and Cushing’s syndrome. Absorption is likely to be greatest where skin is thin, broken and in flexural areas. Local side effects are outlined in Box 9.2.
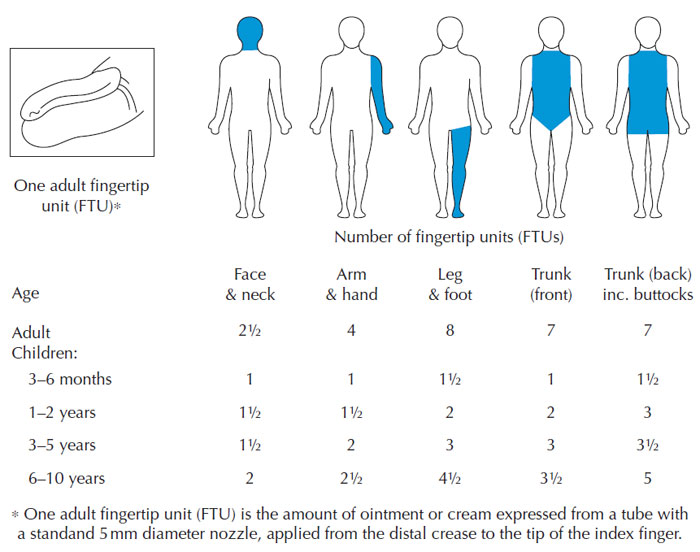
Topical corticosteroid application A practical measure devised for a practical measurement technique for the application of topical corticosteroids is the Finger Tip Unit (FTU) (Long and Finlay, 1991). One FTU is the amount of cream/ointment squeezed from the tip of an adult index finger to the first crease of the finger tip. One FTU (approximately 500 mg) is sufficient to cover an area that is twice that of the flat adult palm. For treating children, an adult FTU is used but the amount of FTUs are reduced depending on the age of the child (see Figure 9.11). The use of the FTU helps patients to understand how much topical corticosteroid to apply to ensure full therapeutic effectiveness. Current treatment guidelines recommend that topical corticosteroids should be stepped up or down according to severity and clinical response (NICE, 2007). Topical corticosteroids should be used to treat inflamed eczema (flare-ups), and in between flares, periods of using emollients only are advised.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
© 2024 Skin Disease & Care | All Rights Reserved.