How is PMLE diagnosed?
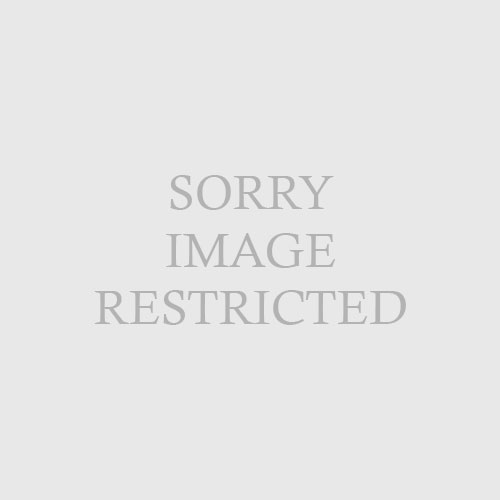
| | Fig. 17.5 Ultraviolet B (UVB) (290 to 320 nm) phototest sites in a patient with polymorphous light eruption demonstrating marked photosensitivity. These test sites were read at 48 hours. (Courtesy of the Fitzsimons Army Medical Center teaching files.) | PMLE is a clinical diagnosis, based on the history of a recurrent photoeruption, usually occurring each spring or early summer, with a consistent skin biopsy. There is no individual clinical, histologic, or laboratory finding that can establish a diagnosis of PMLE. Thus, it is important to exclude other causes of photosensitive dermatoses, such as lupus erythematosus and photodrug eruptions. Generally, the skin biopsy is helpful in this regard. In addition to routine histology, other negative tests include direct immunofluorescence testing of lesional skin (to exclude cutaneous lupus erythematosus), testing for antinuclear antibodies (including anti–Ro/SS-A antibodies), and a porphyrin screen (to rule out erythropoietic protoporphyria). Light testing may demonstrate a lowered minimal erythema dose (MED), that is, the dose of ultraviolet light required to produce erythema is less than one would predict on the basis of skin type (Fig. 17-5).
|