Describe the clinical findings in dermatitis herpetiformis.
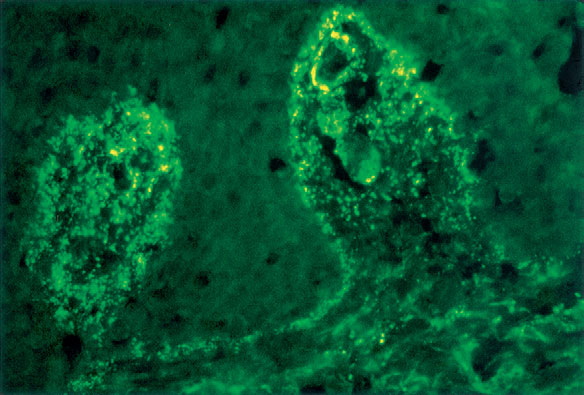
Dermatitis herpetiformis is an autoimmune disease due to IgA autoantibodies directed against tissue transglutaminase. Dermatitis herpetiformis, an extremely pruritic condition, most commonly begins in early adult life and is characterized by symmetrically distributed papules and vesicles that develop on the elbows, knees, buttocks, extensor forearms, scalp, and, sometimes, face and palms (Fig. 10-6). In some patients, the lesions are generalized and severe. Patients may have an associated gluten-sensitive enteropathy, though it is seldom symptomatic. The diagnosis is established by routine histologic exam of an early blister and direct immunofluorescence of nonlesional skin (IgA is seen in the dermal papillae) (see Fig. 10-2). Scratching may destroy all intact blisters for skin biopsy, and thus direct immunofluorescence may be a particularly helpful diagnostic test. Serologic testing for antiendomysial/eTG antibodies and antigliadin antibodies is also a useful screening test. Alonso-Llamazares J, Gibson LE, Rogers RS 3rd: Clinical, pathologic, and immunopathologic features of dermatitis herpetiformis: review of the Mayo Clinic experience. Int J Dermatol 46:910-919, 2007. | ||||
© 2024 Skin Disease & Care | All Rights Reserved.