Antinuclear Antibody (ANA) | Figure 3.31
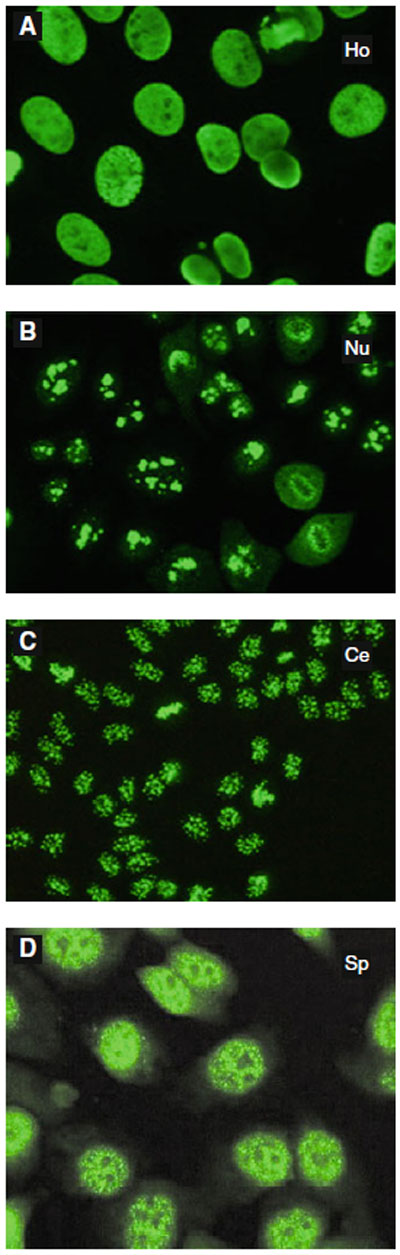
ANA patterns
A: Homogenous*
B: Nucleolar*
C: Centromeric*
*Reprint from Cuenca S, et al.
Rationelle und rationale
Laboratorium diagnostik in der
Hals-Nasen-Ohren-Heilkunde.
HNO. 2008: 56 (9); 855–73
D: Speckled
(Reprint from Vergani D, et al.
Autoimmune Hepatitis. Seminars
in Immunopathology. 2009: 31
(3); 421–435) |
- Family of autoantibodies which may be directed at one or several of the following nuclear antigens:
- Extractable nuclear antigens (ENAs)
- Sm (Smith)
- RNP (U1 ribonucleoprotein)
- Ro (SSA)
- La (SSB)
- Scl-70
- Jo-1
- Non-ENAs
- ds-DNA (double stranded)
- Histone
- Nuclear RNA
- ANA assay measures the amount (titer) and pattern of antibodies in a patient’s serum that bind autoantigens present in the nucleus of cells
- The titer represents the last doubling dilution in order to produce a sample with no fluorescence (ANA-free)
- Two types of assays: indirect IF (IIF) and ELISA
- IIF: most accurate, uses Hep-2 epithelial carcinoma cells as substrate (due to ↑ nuclear/cytoplasmic ratio)
- ELISA: more popular due to decreased cost
- Patterns of nuclear fluorescence if ANA titer positive:
- Homogenous (diffuse) suggests anti-dsDNA (SLE)
- Peripheral (rim) suggests anti-dsDNA (SLE)
- Speckled suggests anti-U1RNP (MCTD, Sjögren)
- Centromeric stains kinetochore (CREST)
- Nucleolar suggests anti-fibrillarin (SSc)
- Five percent of normal population with elevated ANA but nonsignificant; ANA increases with age (i.e. 15% patients >55 years of age with ↑ ANA titer but no clinical significance)
|