Preventing skin damage by scratching
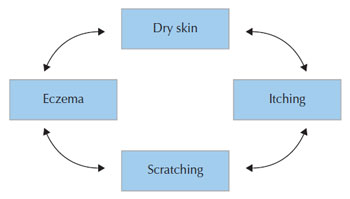
Breaking the scratch–itch cycle and behavioural management A fundamental management problem with eczema is the disruption of the skin barrier due to scratching in response to itch. Itching evokes scratching that further damages the skin leading to more itching, a vicious itch–scratch cycle is established (see Figure 4.1) and therefore breaking this cycle is a primary clinical aim (Hagermark and Wahlgren, 1995). Behavioural management is a strategy that may help manage damaging habit of the itch–scratch cycle. The key principle of classical conditioning views learning as a behavioural response to itch may take place if it is paired with a positive or aversive stimulus. Cognitive behavioural approaches focus on the ability and intention to change behaviour to the benefit of the individual and others. Habit reversal is a well-established method of eliminating nervous habits and tics, whereby an alternative or competing behaviour was adopted in place of the undesirable behaviour (Azrin and Nunn, 1973). The empirical base emerged from the early studies of Azrin. Classic studies include work on nervous habits in adolescents (Allen, 1998; Rapp et al., 1998); these include small numbers of cases and the use of direct observation techniques. One the clearest accounts of habit reversal remains that by Bridgett et al. (1996) in London, based on the work of Melin, Noren and colleagues in Uppsala Sweden, as cited previously (Noren, 1995). They advise that this does not require a trained behavioural therapist – and as such this technique can be used by those that are delivering dermatology care and could be applied for all ages. Miltenberger et al. (1998) provide an overview of the elements of habit reversal and evidence regarding its effectiveness. This paper highlights the mechanisms responsible for its success and its effectiveness in reducing nervous habits, such as scratching, in a replicable way. Research over time has attempted to elucidate the key elements of effectiveness. Miltenberger et al. (1998) summarises these three components as follows, as relevant to the parent–child situation. It comprises of three main elements: awareness raising, introducing a competing response and motivational training to maintain engagement. The book by Bridgett et al. (1996) is a useful and detailed practical guide to supporting adults and children with atopic skin disease through habit reversal. The following outline on the nature of training is focused more on supporting the parent and the child, although of course the same principles apply to adult patients. Awareness training (registration) is concerned with demonstrating the occurrence of the habit and bringing it more closely to the child and parent’s attention. This involves helping them to describe the topography of the behaviour, i.e. identifying when it is about to occur and what antecedent factors are most reliably predicting occurrence. One practical way to implement this is to ask parents to keep a scratch diary to record episodes of when their child scratches and any influencing factor that seems to be implicated. The nurse or dermatologists can review this with the parent and child to raise awareness of how their child is responding to the problem of itch. The next stage (competing response training) involves replacing the damaging behaviour with a new individualised pattern which does not lead to damage to the skin, with the following features: the new behaviour was opposite to the old habit, could be maintained for several minutes and was socially acceptable. Alternative behaviours may include clenching the fists, gently pinching the skin or patting it. The substitute behavioural may be planned as a play activity for children, with a behavioural response linked to a story. Motivational training involves reviewing all ways in which the habit is inconvenient or embarrassing to the child and parent prompting the child to use competing response and praising and encouraging them when successful. They emphasise from clinical experience that habit reversal in this application is only successful when individualised and combined with an effective topical treatment. Key to the success of the approach is the person being enabled to manage their own condition. The approach can be delivered as a group approach to improve cost-effectiveness, as illustrated by Ehlers et al. (1995); this could be adapted to the setting of a nurse-led clinic. Increasingly, computer-based or multimedia educational programmes will promote behavioural treatment and aid in effective self-management through programmed instruction. This represents an area where there is further scope for development and evaluation research. | ||
© 2024 Skin Disease & Care | All Rights Reserved.