|
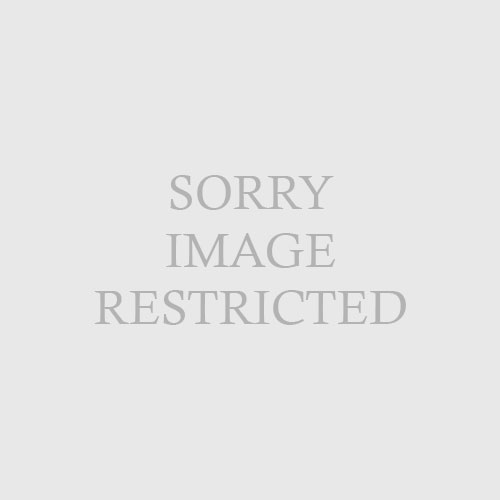
| Fig. 66.3 Young man with factitial panniculitis. The patient was injecting unknown substances into his legs in an attempt to get doctors to provide him with narcotic agents. (Courtesy of James E. Fitzpatrick, MD.) |
|
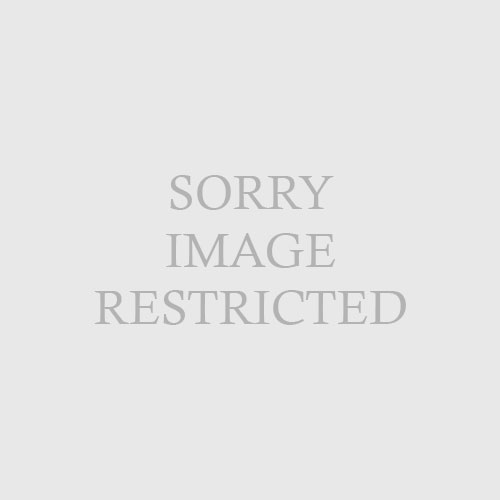
| Fig. 66.2 Patient-induced ulceration and scars of the scalp. |
The self-inflicted lesions vary widely in morphology and distribution. Depending on the method used, it is possible to see blisters from suction cups, burns from caustic chemicals or cigarettes, edema and ulcerations from the use of elastic bands, or deep scars from the use of glass or knives. Lesions are often bizarre and irregularly rectilinear (Figs. 66-2 and 66-3). They are necessarily within reach. Dermatitis artefacta is more common in women.
Koblenzer CS: Dermatitis artefacta: clinical features and approaches to treatment,
Am J Clin Dermatol 1:47–55, 2000.