|
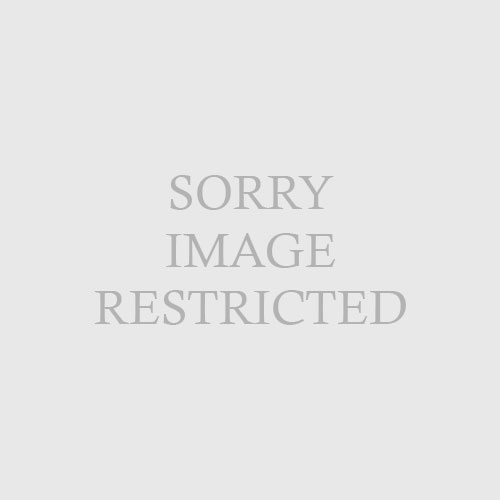
| Fig. 62.6 Annular lichen planus, demonstrating central postinflammatory hypopigmentation. (Courtesy of James E. Fitzpatrick, MD.) |
|
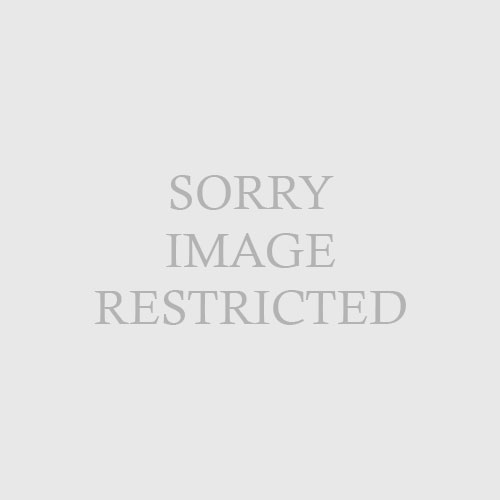
| Fig. 62.5 Tinea versicolor with follicular accentuation. (Courtesy of James E. Fitzpatrick, MD.) |
In addition to the difficulty in perceiving erythema, there exist other cutaneous reaction patterns more prevalent in darker skin. Papulosquamous diseases, such as psoriasis and nummular eczema, tend to exhibit a more violaceous color, leading to possible confusion with lichenoid conditions. Certain diseases, such as atopic dermatitis or tinea versicolor, may demonstrate a follicular accentuation (Fig. 62-5). Pityriasis rosea may present atypically, with either papular or vesiculobullous forms, in black skin. In addition, some disorders, such as lichen planus and seborrheic dermatitis, have an increased propensity toward formation of annular lesions (Fig. 62-6). The reasons for these observations remain largely unknown.
McLaurin CI: Unusual patterns of common dermatoses in blacks,
Cutis 32:352–355, 358-360, 1983.